Fluoroquinolone Tendon Risk Assessor
Evaluate Your Personal Risk
Understand how your age, medical history, and current medications interact.
When Strong Drugs Meet Weak Tendons
You might think taking medicine is always straightforward, but some combinations are far more dangerous than they appear. There is a specific pair of medications that creates a hidden danger for your muscles and joints. When you take Quinolone Antibiotics a class of broad-spectrum antimicrobial agents commonly prescribed for serious infections, your body fights bacteria. But if you are also on Corticosteroids potent anti-inflammatory drugs often used to treat arthritis or asthma, the mix changes completely.
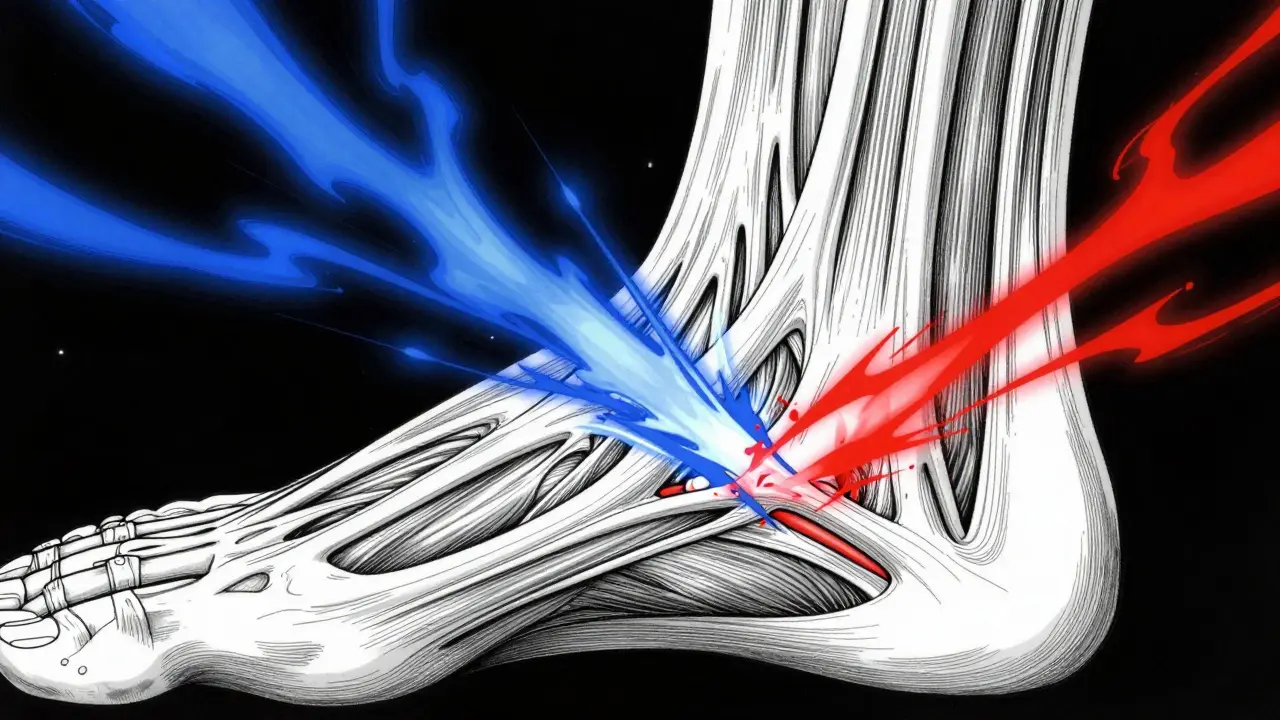
This combination has been linked to a severe condition known as Tendon Rupture the sudden snapping or tearing of a band of tissue connecting muscle to bone. It isn't just a sore ankle; we are talking about a catastrophic injury that can sideline you for months. In fact, one major study found that using these drugs together increases the risk of tendon rupture by 46 times compared to taking the antibiotic alone. That is a massive jump in danger.
The Science Behind the Injury
To understand why this happens, we need to look at what these drugs actually do inside your body. Quinolones work by stopping bacteria from replicating their DNA. They target enzymes called DNA gyrase and topoisomerase IV. While this is great for fighting infection, there is a collateral effect on your own tissue. These antibiotics seem to attack the collagen fibers that hold your tendons together.
Tenocytes are the cells responsible for maintaining healthy tendon tissue. Research suggests that quinolones interfere with tenocyte metabolism. Essentially, the drug weakens the structural integrity of the tendon itself. When you add corticosteroids into the mix, the problem gets worse. Steroids are known to inhibit collagen synthesis and can thin out tissues over time. Together, they create a 'double hit' scenario where the tendon is weakened chemically and then structurally compromised.
This isn't a theoretical risk. A study published in JAMA Internal Medicine highlighted that this adverse effect occurs even after just a single dose of the antibiotic. The damage can happen silently. You might start feeling pain before you ever snap the tendon, but sometimes the rupture is sudden and explosive. The most common location for this disaster is the Achilles Tendon the large tendon located at the back of the ankle that connects calf muscle to the heel bone, though other joints are not immune.
Who Is at Greatest Risk?
Not everyone who takes these meds will suffer an injury, but certain groups face significantly higher odds. Medical databases track thousands of cases to identify patterns. If you fall into these categories, you need to talk to your doctor before starting any fluoroquinolone treatment:
- Age Over 60: Older adults experience a 1.5-fold increase in tendon disorders. Their tendon tissue is naturally less elastic and has lower blood flow, making repair slower.
- Renal Failure: Patients with kidney issues (especially those with glomerular filtration rates under 30 mL/min) retain the drug longer, increasing toxicity levels.
- History of Transplants: People who have had heart, kidney, or lung transplants often take immunosuppressants which include corticosteroids.
- Diabetes Mellitus: Diabetes affects circulation and healing, making tendons more susceptible to damage.
- Previous Ruptures: If you have torn a tendon before, that tissue is already vulnerable.
The risk is especially high when these factors stack up. For example, a 65-year-old patient with asthma taking daily prednisone (a steroid) for an infection treated with ciprofloxacin is in a very high-risk zone.
Timing and Latency of the Injury
One confusing aspect of this injury is the timeline. You might finish your course of medication and still get hurt. Data from the General Practice Research Database shows that the median onset for tendinopathy is about 6 days after starting treatment. However, 85% of cases occur within the first month of therapy.
Here is the tricky part: up to 50% of these injuries develop even after you stop taking the fluoroquinolone. The damage continues to manifest while the drug leaves your system. This means you cannot simply assume you are safe once the prescription bottle is empty. Symptoms can linger or flare up weeks later.
If you are monitoring yourself, watch for a specific latency pattern. Early warning signs usually precede the actual rupture by up to two weeks. Ignoring pain during the first month of treatment is the biggest mistake patients make. By the time the tendon snaps, the warning phase has often passed.
Different Antibiotics Have Different Risks
While all systemic fluoroquinolones carry a black box warning from the FDA regarding tendon rupture, they aren't all equal in their danger profile. Some specific drugs are reported much more frequently in adverse event logs.
| Antibiotic Name | Reported Frequency | Primary Usage | |
|---|---|---|---|
| Ciprofloxacin | Highest (Approx. 68%) | UTI, Skin Infections | |
| Norfloxacin | Moderate (Approx. 30%) | Prostatitis, UTI | |
| Levofloxacin | Lower (Rare reports) | Pneumonia, Respiratory | |
Ciprofloxacin consistently tops the list for tendon-related complaints. However, since levofloxacin is also widely prescribed for respiratory conditions, patients shouldn't consider themselves safe just because they aren't on Cipro. The chemical structure of fluoroquinolones allows them all to bind to the same metabolic pathways involved in tendon health.
Recognizing the Symptoms Early
Catching this issue early can prevent permanent disability. The injury typically presents in stages. It starts with tendinitis-inflammation of the tendon-before progressing to a full tear.
Watch for these specific signals:
- Sudden Pain: Often described as sharp or shooting, occurring even without heavy exertion.
- Swelling: Visible puffiness around the affected joint, particularly behind the ankle.
- Inability to Bear Weight: If you find it painful to stand on tiptoes or climb stairs, that is a red flag.
- "Popping" Sensation: Many patients report hearing or feeling a distinct "pop" followed immediately by a loss of function. This indicates a partial or complete rupture.
Bilateral involvement is surprisingly common. About 50% of cases affect both legs simultaneously. Imagine having trouble standing on either foot. This drastically complicates your mobility and daily life. If you notice one side hurting, check the other side immediately.

FDA Warnings and Regulatory Actions
Regulatory bodies have taken aggressive steps to highlight this risk. The U.S. Food and Drug Administration issued its first safety alert in July 2008. However, public awareness was still low, and adverse events continued to be reported. Consequently, in August 2013, the FDA mandated a strengthened 'black box' warning. This is the highest level of warning the agency can issue for prescription drugs.
The current labeling requires doctors to discuss these risks explicitly with patients. The FDA advisory committee concluded that for uncomplicated infections, the benefits of fluoroquinolones often did not outweigh the risks of disabling side effects like tendon rupture. As a result, prescriptions for these drugs have declined significantly since 2013. Doctors now reserve them for cases where other antibiotics fail or when there is no alternative treatment available.
Despite these warnings, global agencies like the European Medicines Agency and New Zealand's Medsafe continue to monitor the situation closely. Medsafe's 2012 update confirmed that tendon rupture remains a rare but well-documented adverse event, reinforcing the need for vigilance in clinical practice.
Alternatives and Clinical Management
If you fall into a high-risk category, avoiding quinolones is the best strategy. Fortunately, modern medicine offers several alternatives depending on the infection type. Penicillins, cephalosporins, and macrolides generally do not carry the same tendon rupture risk.
If a quinolone is absolutely necessary-perhaps due to severe bacterial resistance-the standard of care involves immediate monitoring protocols. Patients should be educated to stop the drug at the first sign of tendon pain. Continuing the medication through pain signals is a direct path to surgery.
For those who have suffered a rupture, recovery is long and arduous. Orthopedic literature estimates typical recovery periods ranging from 6 to 12 months. Surgical intervention is often required, especially for complete ruptures. Post-surgery rehabilitation involves physical therapy to regain range of motion and strength. It is a significant life disruption that underscores the importance of prevention.
Practical Checklist for Patient Safety
To protect yourself, keep this logic in mind during your next visit to the doctor:
- Disclose Everything: Tell your prescriber about every supplement and medication, including over-the-counter steroids.
- Ask about Age: If you are over 60, ask explicitly if a non-fluoroquinolone option exists.
- Listen to Your Body: Don't push through pain. Report swelling immediately.
- Hydrate and Rest: Avoid excessive stress on the ankle while on medication.
- Check Labels: Look for the bold warning on your pill bottle inserts.
Being proactive saves lives and limbs. The information here isn't meant to scare you away from treating serious infections, but rather to arm you with knowledge so you can make an informed decision alongside your healthcare provider.
How long after stopping the antibiotic does tendon rupture risk remain?
Research indicates that up to 50% of tendon injuries occur after discontinuing the fluoroquinolone. The risk period generally extends for several weeks to a month following the last dose.
Is topical steroid cream safer than oral steroids?
Topical steroids generally pose less systemic risk, but caution is still advised. Systemic absorption can occur, and combined risk assessment should always be done with your doctor.
Does exercise worsen the tendon damage while taking fluoroquinolones?
Yes, vigorous physical activity places mechanical stress on weakened collagen fibers. Patients are advised to avoid strenuous sports while on these antibiotics to reduce the chance of rupture.
Can I take NSAIDs like ibuprofen along with these drugs?
NSAIDs have also been associated with increased tendon rupture risk. Combining NSAIDs with fluoroquinolones may further elevate the danger, so consult a physician before mixing these classes.
What is the absolute risk percentage for developing tendon issues?
While relative risk is high with certain combos, the absolute incidence is estimated between 0.1% and 0.4% of all treated patients. It is rare, but the consequence of rupture makes the small risk significant.
Victor Ortiz
March 30, 2026 AT 09:21The statistics are glaringly obvious yet the medical industry continues to push these combinations without adequate oversight.
You see the patterns in the database but patients rarely access the raw numbers before swallowing a pill.
Amber Armstrong
March 31, 2026 AT 00:21It is really heartbreaking to read about this.
So many people get hurt just trying to feel better from an infection.
The way these drugs combine is so scary honestly.
You would think the warnings were enough for everyone.
But nobody checks the labels anymore these days.
My cousin went through something similar last year.
She was taking steroids for asthma constantly.
Then they gave her the antibiotic for a lung thing.
One day she just fell down while gardening.
The pain was instant and absolute in her ankle.
It took forever for her to walk properly again.
Surgery was painful and rehab was tough.
She hates how vulnerable her legs felt afterwards.
We just need to be more careful reading the inserts.
Listening to bodies matters more than trusting pills blindly.
Hope everyone stays safe here.
Cameron Redic
April 1, 2026 AT 11:05People ignore warnings until their legs snap.
Ruth Wambui
April 2, 2026 AT 12:41Pharmaceutical giants hide these side effects until the lawsuits become impossible to ignore completely.
William Rhodes
April 3, 2026 AT 10:41Knowledge is power but ignoring it leads to broken bones and wasted years of recovery.
We must take responsibility for our own treatment plans regardless of what the doctor prescribes.
If you do not ask the hard questions then you are not fighting for your health.
Brian Yap
April 3, 2026 AT 12:22G'day mate, reckon this applies globally even down under where we sometimes lag on safety updates.
Katie Riston
April 5, 2026 AT 04:58There is a profound fragility inherent in the human condition when chemical interactions become unpredictable variables in our biology.
We trust systems designed by fallible minds to protect our physical integrity during illness.
Yet those very systems introduce new risks that compound existing vulnerabilities we never anticipated having to manage.
The tendon represents a connection between muscle and bone but also symbolizes the link between mind and body action.
When that link fails silently under pressure it forces a reevaluation of how we view medical progress.
We celebrate curing infections while overlooking the cost paid in structural damage to our locomotion.
This trade off seems unfair given that modern medicine promises safety above all else.
Carolyn Kask
April 6, 2026 AT 09:27Oh great another American FDA scare story nobody will actually listen to.
Michael Kinkoph
April 7, 2026 AT 23:23This is definitely true!!! And the regulations are clear!!! Why do people ignore them??? It is negligence plain and simple!!!
Marwood Construction
April 9, 2026 AT 13:57Clinical guidelines remain consistent regarding contraindications for high-risk patient populations involving renal failure.
Biraju Shah
April 9, 2026 AT 14:28Guidelines mean nothing if ignored.
Jonathan Alexander
April 10, 2026 AT 17:55I lost my father to exactly this tragedy.